In today’s world of selfies and smartphones, a beautiful smile is desired by all. People have become more aesthetically conscious and have begun to seek orthodontic treatment to correct the malocclusion in their dentition and improve aesthetics. A beautiful smile is a pleasure to the eyes and orthodontics is the branch of dentistry which provides people with the smile they want.
In the growing age, children encounter a variety of dento-facial abnormalities and malocclusion. It is important to identify the malocclusion and correct it at the right age for proper development of the dento- facial structures. Malocclusions hamper the aesthetics of a person as well. Thus, it is necessary that the abnormality is addressed on time.
There are certain deleterious oral habits which the children acquire at an early age and this leads to malocclusions.
It is important to intercept these habits at the earliest.
Proper oral hygiene habits should be instilled in children at an early age to avoid dental caries and periodontal diseases. Dental caries and periodontal diseases can lead to premature loss of deciduous as well as permanent teeth leading to malocclusions.
Here are a few points which will improve our understanding about orthodontics and the oral habits in growing children.
The need for the correction of malocclusion:
An incorrect bite can lead to:
- Interference with normal growth and development of jaws
- Impaired chewing
- Difficulty swallowing
- Speech defects
- Malocclusion makes the person more susceptible to cavities and periodontal problems
- Poor esthetics
- Deleterious oral habits in growing children:
The American Academy of Pediatric Dentistry (AAPD) recognizes that an infant’s, child’s, or adolescent’s well-being is affected by oral habits and encourages health practitioners to take an individualized approach in the management of these habits.
Frequently, children acquire certain habits that may either temporarily or permanently be harmful to dental occlusion and to tooth supporting structures.
The different deleterious oral habits and their treatment is discussed below:
Thumb and digit sucking:
- Placement of thumb or one or more fingers in varying depths into the mouth.
- One of the most commonly seen habits.
- The presence of this habit is considered quite normal till 3.5 to 4 yrs of age.
Clinical features
Proclination of maxillary anterior
Increased over jet
Anterior open bite
Narrow maxillary arch: The muscles contract during thumb sucking leading to a narrow maxillary arch
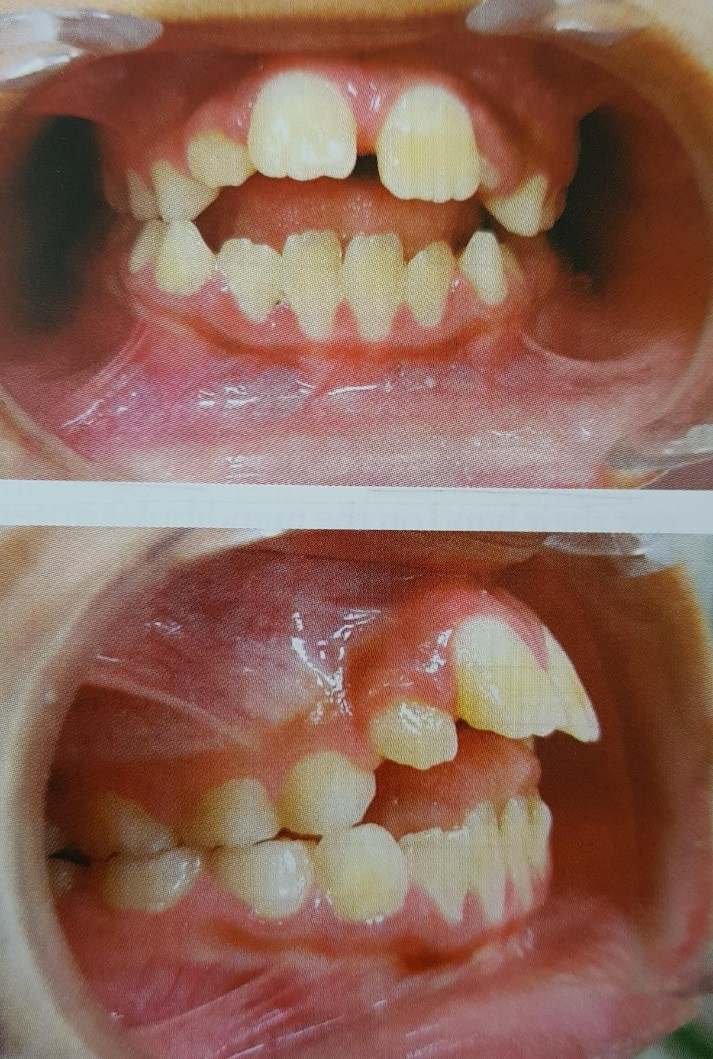
(Photograph of an eight year old patient with thumb sucking habit.)
Diagnosis: Presence of clean nails and callus on the finger is commonly associated with thumb sucking
Management: There are three approaches in the management of thumb sucking.
- Psychological
- Mechanical
- Chemical
1. Psychological: Thumb sucking is said to be attributed to lack of love, parental care and affection.
The parents should be counselled to provide the child with adequate love and care. The attention of the child should be diverted to other things such as games and toys.
Dunlop beta hypothesis: Dunlop put forward a theory that states the best way to break a habit is by its conscious, purposeful repetition. Dunlop suggests that the child should be asked to sit in front of a large mirror and asked to suck his thumb observing himself.
2. Mechanical: They are reminding appliances that help the child quit the habit.
They can be removable or fixed.
 Palatal crib
Palatal crib  blue grass appliance
blue grass appliance
3. Chemical: Placing bitter tasting preparations on the thumb that is sucked can make the habit distasteful.
- Pepper dissolved in a volatile medium
- Quinine
- Asfoetida
- Femite
Tongue thrust habit
Condition in which the tongue makes contact with any teeth anterior to the molars during swallowing.
Clinical features
- Proclination of anterior teeth
- Anterior open bite
- Bomaxillary protrusion
- Posterior open bite in case of lateral tongue thrust
- Posterior cross bite
Management of tongue thrust
Habit interception:
1. Habit breaker appliances – fixed or removable cribs and rakes
2. The child is taught the correct method of swallowing
3. Various muscle exercises of the tongue :
The hold pull exercise: The tip of the tongue and the midpoint are made to contact the palate and the mandible is gradually opened. This helps in stretching the lingual frenum.
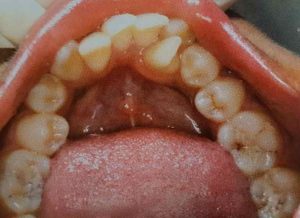
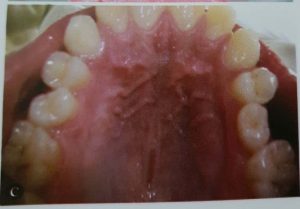
Mouth breathing habit
Mouth breathing can result in altered jaw and tongue posture, which could alter the oro-facial equilibrium thereby leading to malocclusion.
Types of mouth breathers:
- Obstructive
- Habitual
- Anatomic
1. Obstructive: Complete or partial obstruction of the nasal passage can result in the mouth breathing. Some causes of nasal obstruction are:
- Deviated nasal septum
- Nasal polyps
- Chronic inflammation of nasal mucosa
- Localized benign tumors
- Obstructive adenoids
2. Habitual: A habitual mouth breather is one who continues to breathe through his mouth even though the nasal obstruction is removed.
3. Anatomic: An anatomic mouth breather is one whose lip morphology does not permit complete closure of the mouth such as patient having short upper lip.
Clinical features
- Long and narrow face
- Narrow nose and nasal passage
- Short and flaccid upper lip
- Contracted upper arch with possibility of posterior cross bite
- Increased over jet as a result if flaring of upper incisors
- Anterior marginal gingivitis can occur due to drying of the gingiva
- Dry mouth predisposing to caries
- Anterior open bite

Patient with mouth breathing exhibiting marginal gingivitis.
( source: textbook of orthodontics by S.I BHALAJI )
Management
1. Removal of the nasal or pharyngeal obstruction
2. Interception of the habit: use of vestibular screen
3. Rapid maxillary expansion: patients with narrow, constricted maxillary arches benefit from expansion procedures aimed at widening the arch. It has been found to increase the nasal airflow and decrease the nasal air resistance.
Bruxism
Bruxism can be defined as the grinding of teeth for non functional purposes. Some authors refer to nocturnal grinding as bruxism and bruxomania is the term given for grinding during day time. Psychological and emotional stresses have been attributed as one if the major causes in bruxism.
Clinical features
- Oclussal wear facets.
- Fractures of teeth and restorations.
- Tenderness and hypertrophy of masticatory muscles.
- Headache and pain in the facial muscles when the patient wakes up in the morning.
Management
- As stress is the major factor, appropriate counseling by a psychiatrist maybe initiated.
- Hypnosis, meditation and relaxing exercises can help in relieving muscle tension.
- If occlusal prematurities are present , occlusal adjustments can be made.
- Night guards help in eliminating occlusal interference and prevent occlusal wear.
Lip biting
Lip biting and lip sucking sometimes appear after forced discontinuation of thumb or finger sucking. It most often involves the lower lip that is turned inwards and pressure exerted on the lingual surface of the maxillary anterior.
Clinical features
- Proclined upper anteriors and retroclined lower anteriors
- Hypertrophic and redundant lower lip
- Cracking of lips
Management
This habit can be intercepted using lip bumpers.
The different malocclusions occurring in children are of a number of types.
To make our understanding easier they can be broadly divided into: intra-arch , inter arch and skeletal.
1. Intra-arch: The malocclusions occurring within the same arch either the maxilla or mandible

- Distal tipping
- Mesial tipping
- Lingual tipping
- Buccal tipping
- Spacing between teeth

- Crowding : Lack of space leads to crowding and ectopic eruption the teeth
- Rotations
2. Inter-arch: When there is discrepancy in the relationship between the maxillary and mandibular teeth.
- Deep bite: It is a condition in which there is excessive vertical overlap between the maxillary and mandibular anteriors.

- Open bite : A condition in which there is no overlap between the maxillary and mandibular anteriors.
- Cross bite which can be anterior or posterior : It is the abnormal transverse relationship between upper and lower arches.

3. Skeletal: Skeletal malocclusions that involve abnormalities in the maxilla or mandible. The defects can be in size, position or relationship between the jaws. The maxilla or mandible can either be deficient or excessive in its size.
When is the best time for orthodontic treatment?
- The jaws of pre–teens and teens are still growing. Therefore, it is easier to shift teeth at this age.
- Sometimes two separate phases of braces are necessary.
- Phase 1 : when patients are 6 -7 years of age to amle room for the permanent teeth
- Phase 2 : at age 12 (when all the permanent teeth have erupted) second round of braces are applied to straighten the teeth and correct the bite.
- We are living in a world where people are conscious and concerned about their appearance and specially their smile. As a result more and more adults also seek orthodontic treatment. The treatment may take a longer time in adults.
As we discuss the different malocclusions and the best time for the treatment, it might occur to us what can cause malocclusion in the first place.
What causes malocclusion?
- Genetics: One may inherit a small jaw from the mother and large teeth size from the father.
- Nutritional deficiencies: Malnutrition can restrict the growth of the jaws
- Bad oral habits can cause a shift in the normal position of the teeth or can cause them to erupt abnormally. The various deleterious habits have been discussed later.
- Tooth loss: If a tooth is lost either due to trauma, caries or periodontal disease, the rest of the teeth may shift. Premature loss or prolonged retention can also lead to a deviation in the path of eruption of the succedaneous tooth.
- While some forms of malocclusion are inherited and unavoidable, a variety of malocclusions can also be prevented by taking the right measures at an early age and intercepting the deleterious oral habits. It is also true that whatever may be the type of malocclusion or abnormality in the dentition, it can be treated by an orthodontist.
- Along with intercepting the deleterious oral habits, it is also essential to inculcate good oral hygiene habits in children at a young age.
1. Brush twice daily: In the morning and at night before going to bed
2. Rinse your mouth after every meal
3. Decrease the frequency of sugary foods
4. Children should floss at least once a day. Young children will need supervision from the parents
5. Regular dental check ups every 6 months.
Take home message: Malocclusion can affect the growing children and lead to aesthetic as well as functional abnormalities. It is very important to seek orthodontic treatment at an early age to gain best results. The parents should pay attention to any oral habits that the child may acquire and seek help of a dentist to get rid of them. Parents should instill good oral hygiene habits in the children and should understand the importance of regular dental checkups. Remember, a smile is valuable.
Leave a Reply